
The Impact of Opioid Use on NeoNatal Health
The surge in opioid use across the United States has not only affected adults but has also significantly impacted neonatal health, as chronic exposure to opioids during pregnancy adversely affects fetal and placental development (Figure 1) (5, 6). Fundamental developmental and biological processes are disrupted which severely hinder long-term brain growth in infants. Studies indicate opioids may alter placental function and structure, leading to complications such as fetal growth restriction and preterm labour (5). Neonatal Abstinence Syndrome (NAS) is a multisystemic disorder experienced by newborns with mothers who took opioids or other substances while pregnant.6 NAS occurs when newborns withdraw from drugs such as opioids, resulting in hyperactivity of the gastrointestinal tract as well as the autonomic and central nervous systems (3,5). Approximately 60–80% of infants exposed to opioids develop Neonatal Abstinence Syndrome (NAS) and are at risk of neurodevelopmental morbidity; if untreated, this condition can lead to death. With opioids ranging from illicit drugs like heroin or morphine to legally prescribed medications such as buprenorphine and methadone, the incidence of NAS has seen a dramatic rise in recent years (1, 6). From 1999 to 2014, NAS rates increased from 1.5 to 14.4 cases per 1000 hospital newborns.6 Not to mention, the frequency of opiate usage during pregnancy has climbed by 333% in the US and is still rising (1). NAS leads to various clinical signs and symptoms in infants, including sleep and behavioural problems, irritability, hypertonicity, sneezing, seizures, tremors, vomiting, diarrhea and failure to thrive (1,3,6). Moreover, NAS induces deficits in several neurodevelopmental domains, including cognition, language, and motor. Understanding the link between opioid use and NAS is crucial for implementing effective interventions to mitigate its impact on neonatal health (6)

Figure 1: The yearly count of Neonatal Abstinence Syndrome (NAS) births in the United States from 2008 to 2017 (5).
A recent cross-sectional state-level ecologic analysis sought to delve into the relationship between opioid use and NAS, shedding light on various factors influencing its prevalence. The study examined data from pediatric discharge records alongside state-level variables such as substance use disorder treatment access, opioid prescribing rates, demographic characteristics, and NAS incidence rates (Figure 2). Utilizing datasets from sources including the Healthcare Cost and Utilization Project's State Inpatient Databases (HCUP SID), the National Survey on Drug Use and Health (NSDUH), the Substance Abuse and Mental Health Services Administration, the Drug Enforcement Administration (DEA) database, and the U.S. Census Bureau, the analysis provided a comprehensive assessment of the associations between opioid use, treatment access, and NAS incidence. By incorporating diverse data sources, the study aimed to elucidate the complex interplay between these variables and contribute to a deeper understanding of the factors driving NAS prevalence at the state level (6).

Figure 2: Measurements of Opioid Use, Access, Demographics and Outcome (6).
The findings of the cross-sectional state-level ecologic analysis revealed a positive correlation between NAS incidence and measures of adult opioid use, including rates of illicit drug dependence or abuse and opioid prescribing. Furthermore, states with higher proportions of individuals living in rural areas exhibited higher NAS rates, highlighting geographical trends in NAS prevalence. The study also uncovered intriguing insights into the role of opioid use disorder treatment access in mitigating NAS incidence. The unmet need for substance use disorder treatment was found to be positively correlated with NAS, underscoring the importance of improving access to comprehensive treatment programs. Importantly, the correlation between adult illicit drug use and NAS was attenuated in states with higher levels of opioid use disorder treatment access.6 Additionally, a matched cohort study compared the impact of in-utero opioid exposure on newborns in South-Central Appalachia, encompassing 300 prenatal opioid-exposed newborns and 300 control newborns. Various metrics were used to define opioid exposure, resulting in significant differences between the exposed and control groups. Opioid-exposed newborns exhibited increased fetal growth restriction rates, lower birth weights, shorter lengths, and smaller head circumferences along with higher rates of intrauterine growth restriction (IUGR), respiratory distress, neonatal jaundice, and sepsis, compared to controls (Figure 3) (2). These findings corroborate the importance of supporting clinical screening and treatment choices to improve health and well-being before, during, and after pregnancy and highlight the need for comprehensive strategies to tackle NAS (2,6).
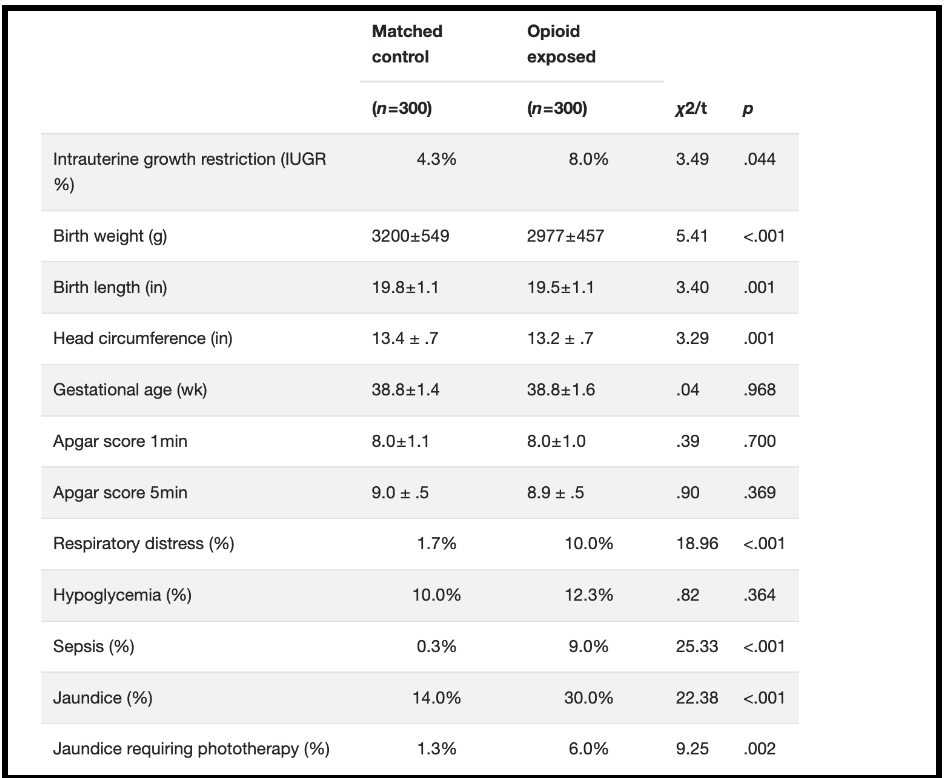
Figure 3: Primary outcome differences between opioid-exposed and matched control groups, obtained through bivariate analysis (2).
Moving forward, efforts to address the impact of opioid use on neonatal health should prioritize strategies aimed at expanding access to comprehensive opioid use disorder (OUD) treatment. This includes increasing the availability of buprenorphine-waivered physicians, enhancing outpatient treatment programs, and providing comprehensive prenatal care and support services for pregnant individuals with opioid use disorders (6). Pharmacological approaches play a crucial role in addressing OUD before, during, and after pregnancy. Treatment plans may include medications for OUD (MOUD) like buprenorphine or methadone, which can significantly increase the number of healthy pregnancies. It is essential to carefully weigh the risks and benefits of starting or continuing opioid medications for chronic pain during pregnancy, with decisions made collaboratively between healthcare providers and patients. Close collaboration between healthcare providers and pediatric teams is vital to monitor newborns for NAS and ensure timely treatment. Postpartum support is crucial for individuals in treatment for OUD, as continued access to healthcare and MOUD alleviates the risk of relapse and overdose events during this vulnerable period (3).
Additionally, initiatives to promote awareness and education among healthcare providers regarding the management of NAS and the importance of early intervention are essential.6 In alignment with these goals, the Mainstreaming Addiction Treatment (MAT) Act provision represents a pivotal step in combating the opioid epidemic. The MAT Act empowers all healthcare providers with a standard controlled substance license to prescribe buprenorphine for opioid use disorder (OUD), thereby destigmatizing a standard of care for OUD and integrating substance use disorder treatment across healthcare settings. As of December 2022, the MAT Act has eliminated the DATA-Waiver (X-Waiver) program, allowing all DEA-registered practitioners with Schedule III authority to prescribe buprenorphine for OUD if permitted by applicable state law. Moreover, the MAT Act removes the patient limit previously imposed on practitioners, enabling them to treat as many patients with OUD as deemed appropriate without the need for separate tracking of patients treated with buprenorphine or prescriptions written (1).
Furthermore, non-pharmacological management of NAS is paramount, beginning with the nurturing of the mother-infant dyad and extending beyond hospital discharge. These approaches focus on aiding the neonate's self-organization and neuro-maturation. Techniques involve modifying the physical environment, such as dimming lights and minimizing noise, to reduce stimuli. Comfort measures like gentle rocking, swaddling, and skin-to-skin contact can soothe irritability and hypertonicity, while frequent, small-volume feeding addresses feeding difficulties and prevents hunger-induced agitation. Individualized care tailored to the infant's needs is crucial, with healthcare providers engaging mothers in identifying effective interventions. Parental rooming-in facilitates increased skin-to-skin contact and breastfeeding, leading to benefits such as reduced hospital stays and decreased reliance on pharmacological treatments, underscoring the significance of non-pharmacological approaches in NAS management (1).
By addressing the root causes of opioid use and implementing targeted interventions, we can strive towards improving neonatal health outcomes and mitigating the impact of NAS on vulnerable newborns and their families (6). Neonatal Abstinence Syndrome (NAS) is a growing concern and has become more prevalent over the years. We must work together to tackle this issue, which can be achieved through initiatives such as raising awareness and educating healthcare providers about pharmacological and nonpharmacological approaches to management, and expanding access to comprehensive opioid use disorder (OUD) treatment (1, 3, 6) Clinical and preclinical research that focuses on the role of the placenta concerning neurobehavioral and neurodevelopmental risks secondary to in-utero exposure must also be conducted to develop preventive and effective fetal/placental therapies (5). Together, we can save the lives of newborns and allow them to thrive and live healthy, fulfilling lives.
References
(1) Anbalagan, S., & Mendez M. D. Neonatal Abstinence Syndrome. (2023, July 21). StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov
(2) Bailey, B. A., Shah, D. S., Boynewicz, K. L., Justice, N. A., & Wood, D. L. (2022). Impact of in utero opioid exposure on newborn outcomes: beyond neonatal opioid withdrawal syndrome. The Journal of Maternal-Fetal & Neonatal Medicine, 35(25), 9383–9390. https://doi.org/10.1080/14767058.2022.2035713
(3) Centers for Disease Control and Prevention. (2022, November 28). About Opioid Use During Pregnancy. https://www.cdc.gov
(4) HCUP. (2020, January 17). Neonatal Abstinence Syndrome Births: Trends in the United States, 2008-2019. https://hcup-us.ahrq.gov
(5) Humphries, A., Simcox, K., & Howell, B. (2023). A review of the literature: How does prenatal opioid exposure impact placental health and fetal brain development? Developmental Psychobiology, 65(3), n/a-n/a. https://doi.org/10.1002/dev.22378
(6) Wolf, E. R., Tong, S. T., Sabo, R. T., Woolf, S. H., Abbinanti, K., Pecsok, J., & Krist, A. H. (2019). A state-level study of opioid use disorder treatment access and neonatal abstinence syndrome. BMC Pediatrics, NA. https://link-gale-com.libaccess.lib.mcmaster.ca